|
Chronic Superficial Keratitis
RESEARCH ARTICLE
Daniel Uribe-Castillo1
1 Department of Veterinary Ophthalmology, Mascotas Centro de Especialistas, Manizales, Colombia
This email address is being protected from spambots. You need JavaScript enabled to view it.
Received: 12 october de 2018 and Approved: 16 january 2019, Updated: 16 june 2019
DOI: 10.17151/vetzo.2019.13.2.3
SUMMARY. Introduction: Chronic superficial keratitis is an inflammatory disease in canines, especially German Shepherds, that progresses by irritative stimuli such as ultraviolet radiation and dust. It presents a favorable prognosis for vision and eye comfort from an early diagnosis approach and an adequate therapeutic plan. Multiple treatment options have been proposed demonstrating that anti-inflammatory and immunomodulatory eye drops are highly effective. Patient and methods: Herein we report the clinical case of a 5-year-old German Shepherd with chronic superficial keratitis. Conclusion: topical prednisolone and cyclosporine and avoidance of ultraviolet radiation resulted in clinical improvement of this patient.
Key words: inflammatory, immunomodulatory, keratitis, ultraviolet
Queratitis Superficial Crónica
RESUMEN: Introducción: La queratitis superficial crónica del ovejero alemán es una enfermedad inflamatoria acelerada por estímulos irritativos como la radiación ultravioleta y el polvo, presenta un pronóstico favorable para la visión y el confort ocular a partir de un abordaje diagnóstico precoz y un adecuado plan terapéutico. Se han planteado múltiples opciones de tratamiento para la condición, demostrándose que los colirios antiinflamatorios e inmunomoduladores tienen gran efectividad. Paciente y métodos: el presente artículo muestra el caso clínico de un canino de 5 años con queratitis superficial crónica. Conclusiones: La prednisolona y ciclosporina tópica, además de prevención de radiación ultravioleta produjeron mejoría clínica del paciente.
Palabras clave: inflamatoria, inmunomodulador, queratitis, ultravioleta.
Introduction
Chronic superficial keratitis (CSK) of canines, formerly known as Pannus or Uberreiter’s Syndrome, classically presents as a corneal fibrovascular lesion (Gellat et al., 2014) with bilateral growth of vascular inflammatory tissue originating from the corneoscleral limbus. CSK is an inflammatory disease that usually affects German Shepherds, Belgian Shepherds, and their crosses. However, similar characteristics have been reported in Greyhounds, Shetland Sheepdogs, Siberian Huskies, Scotch Collies, Border Collies, Australian Shepherds, and Dachshunds (Martin, 2010).
A progressive lesion and inflammatory behavior have the potential to cause visual loss in canines (Samuelson & Brooks, 2011). The clinical picture usually starts from the inferior and temporal quadrants of the cornea, and the inflammatory and pigmentation process progresses to the rest of the cornea. Over time, the chronic disease can begin from the nasal sclerocorneal limbus. Similar to multiple diseases that involve superficial corneal vascularization, limbal melanocytic migration occurs in CSK. The upper portion of the cornea is usually intact during the early stages. Some canines may develop further inflammation as well as conjunctival and nictitating membrane pigmentation (Gellat et al., 2014).
The exact cause is unknown, although cellular immunity to corneal and uveal antigens has been demonstrated, as observed in other chronic corneal pathological processes. During the early stages, epithelial cells proliferate and the superficial stroma is infiltrated by plasma cells and lymphocytes. As the condition persists, cells such as melanocytes, histiocytes, and fibrocytes also penetrate the cornea. During the advanced stages, the epithelium and superficial stroma are strongly pigmented and vascularized. Generally, the corneal epithelium remains intact throughout the duration of the condition, but during the inflammatory stage, there may be granulation tissue that generates positive fluorescein staining (Maggs et al., 2013). Corneal lipid deposits may be observed, but ulcerative keratitis is rare (Petersen & Crispin, 2002). It is believed to be due to hypersensitivity to corneal proteins induced by environmental factors such as ultraviolet (UV) light, dust and wind. The most common age of presentation is between 2 and 7 years (Herrera, 2007). Animals with greater exposure to UV radiation exhibit more severe clinical signs (Maggs et al., 2013). Studies have shown that canines that live at altitudes above 7000 feet above sea level are 7.7 times more susceptible to CSK than those that live at lower altitudes (Gellat et al., 2014).
CSK is categorized into two stages according to its clinical signs. The first is an active stage of acute inflammatory processes with irritative signs such as epiphora and blepharospasm and the predominance of infiltrative growth. The second stage is the sequel and is characterized by the deposition of corneal melanin pigments. In addition, each stage can be subdivided into three subcategories (1–3) according to the third of the corneal diameter that the lesion covers (Herrera, 2007).
Diagnosis of the disease is generally presumptive when bilateral proliferative keratitis is presented in a predisposed breed, in addition to the response to anti-inflammatory therapy (Martin, 2010). Cytology usually shows lymphoplasmacytic cells (Maggs et al., 2013). Histopathological studies of affected corneas have revealed the infiltration of abundant blood vessels, lymphocytes, and plasma cells in the corneal stroma.
Pigmentary keratitis resulting from other causes of chronic irritation such as trichiasis, keratitis sicca, and scar granulation should be ruled out (Gellat et al., 2013).
The traditional treatment consists of the administration of topical, subconjunctival, or systemic steroids according to the degree of condition. In addition, techniques such as a superficial keratectomy for sequential stages are indicated (Herrera, 2007). Treatments with cyclosporine, tacrolimus, and pimecrolimus have demonstrated efficacy for treating CSK. Additional therapies such as cryotherapy and beta radiation have been used to remove and disperse the corneal pigment, in addition to suppressing inflammation in cases where steroid management is difficult (Martin, 2010).
The therapeutic objective is to generate regression of the lesion to avoid blindness. The frequency of topical therapy is usually reduced as clinical signs are controlled (Maggs et al., 2013). The prognosis for preserving vision and controlling the disease might be unfavorable in those animals that show an accelerated evolution; however, most affected dogs have a positive response to anti-inflammatory and immunosuppressive treatment (Dubielzig et al., 2010). Thus, the disease can be controlled but not cured (Samuelson & Brooks, 2011).
Patient Evaluation
Case History
A 5-year-old German Shepherd presented for a consultation due to bilateral corneal lesions that caused ocular discomfort (blepharospasm and epiphora) for 2 months. The canine resided in a rural area in the outskirts of the city, and the owners reported that the patient endured long days under intense sunlight.
Clinical findings
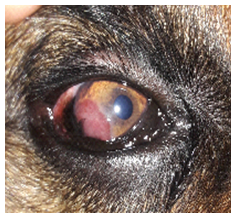
The systemic condition of the patient did not show signs of any additional pathology and the ophthalmological evaluation also did not show any other alterations. Tear production in both the eyes was in the normal range of the Schirmer I test (Merck Animal Health, Summit, NJ, USA). The fluorescein test (Bioglo Ophthalmic Strip, CA, USA) was negative for both the eyes. Denture tonometry revealed the intraocular pressure of 23.8 and 20.1 mmHg for the right and left eyes, respectively. The evaluation of posterior segments and fundoscopy did not show any abnormalities. Corneal evaluation identified a bilateral corneal lesion starting in the inferotemporal quadrant with vascular characteristic in the form of a granuloma (Figures 1 and 2). In addition, the patient presented with mild conjunctival congestion and moderate epiphora and blepharospasm. The diagnosis was active stage 1 CSK due to the acute inflammatory phase and corneal invasion.
Figure 1. The right eye inflammatory lesion originating from the inferior temporal limbus
Figure 2. The left eye inflammatory lesion originating from the inferior temporal limbus
Therapeutic approach
Prednisolone acetate 1% (Pred F®, Allergan, Colombia) and cyclosporine 1% (Holliday, Argentina) were topically administered thrice a day. Furthermore, the avoidance of prolonged exposure to solar radiation using canine UV protection lenses was recommended (Figure 3).
Figure 3. The patient with UV protection glasses
Reassessment of the patient after 30 days of treatment revealed total improvement of the initial signs present during the consultation, in addition to the disappearance of the corneal vascular tissue that was replaced by melanin pigmentary tissue (Figures 4 and 5). Due to the incurable nature of the disease, six-monthly checks were indicated to prevent relapses and to reduce the risk of visual loss.
Figure 4. Right eye corneal scar pigment tissue
Figure 5. Left eye corneal scar pigment tissue
Discussion
Previously, CSK was considered as a pathology without predilection for gender (Herrera, 2007), but studies have shown that females have a higher prevalence of the pathology (Gellat et al., 2013). Immunohistochemical studies have suggested that the condition is not an autoimmune process but an inflammatory one that is mediated by perilimbal lymphatic tissue cells, probably under the stimulation of UV light (Herrera, 2007).
A previous study compared three groups and three treatments for the active stage of CSK. The first group was treated with topical, subconjunctival, or systemic steroids only, the second group with cyclosporine, and the last group was treated with a mixture of steroids plus cyclosporine. Group 3 was the one that showed the best results, whereas the second group showed the worst results (Herrera, 2007).
Conclusion
CSK is an incurable ocular pathology, but with opportune treatment, it can have a favorable visual and ocular comfort prognosis. It is important to recognize the characteristic clinical condition and from its classification, suggest the best treatment for the respective case. In addition, it is important to inform the owners that the disease is incurable and that the animal will require treatment for the rest of its life.
Bibliographical references
Dubielzig, R.; Ketring, K.; McLellan, G.; Albert, D. Diseases of the cornea and sclera. Veterinary ocular pathology a comparative review. Saunders Elsevier, St. Louis, p. 212-213. 2010.
Gellat, K. Canine cornea: diseases and surgery. Essentials of veterinary ophthalmology, 3th ed. Wiley Blackwell, Iowa, p. 237-238. 2014.
Gellat, K.; Gilger, B.; Kern, T. Diseases and surgery of the canine cornea and sclera. Veterinary ophthalmology, 5th ed. Wiley Blackwell, Iowa, p. 1012-1013. 2013.
Herrera, D. Enfermedades de la córnea. Oftalmología clínica en animales de compañía. Inter-médica, Buenos Aires, p. 126. 2007.
Maggs, D.; Miller, P.; Ofri, R. Cornea and sclera. Slatter´s fundamentals of veterinary ophthalmology, 5th ed. Elsevier, St. Louis, p. 205-206. 2013.
Martin, C. Cornea and sclera. Ophthalmic disease in veterinary medicine. Manson, London, p. 257-258. 2010.
Petersen, S.; Crispin, S. BSAVA manual of small animal ophthalmology, 2nd ed. BSAVA, Gloucester, 143p. 2002.
Samuelson, D.; Brooks, D. Small animal ophthalmology. Manson, London, 52p. 2011.
Como citar: Uribe-Castillo, D. Queratitis superficial crónica. Revista Veterinaria y Zootecnia, v. 13, n. 2, p. 24-30, 2019. http:// vetzootec.ucaldas.edu.co/index.php/component/content/article?id=274. DOI: 10.17151/vetzo.2019.13.2.3
Esta obra está bajo una Licencia de Creative Commons Reconocimiento CC BY
|






 | Today | 100 |
 | Yesterday | 351 |
 | This week | 451 |
 | Last week | 3121 |
 | This month | 10484 |
 | Last month | 18517 |
 | All days | 1373615 |
Online Now: 20
Your IP: 18.226.187.60
MOZILLA 5.0,
Today: December 24, 2024
Your IP: 18.226.187.60
MOZILLA 5.0,
Today: December 24, 2024